
It was nearing the end of the rainy season in 1973, and the road was washed out. So to reach our destination that day, we had to walk along a quarter mile of rice paddy dykes while humping our equipment and supplies. Our objective was a large cluster of trees in the middle of several paddies in the Tha Rae district of Sakon Phanom Province of northeast Thailand.
Nestled in among those trees was a Catholic church and orphanage run by a Thai priest and staffed by Thai nuns. I was naively unaware of that until we arrived, and was surprised to see nuns in their habits in the middle of a Buddhist country. Our mission was to provide primary medical care to the orphanage children.
My tour of duty in southeast Asia during the Vietnam War was at Nakon Phanom Royal Thai Air Force Base, known to those of us who served there as ‘Naked Fanny’. The base was 14 miles west of the town of Nakon Phanom, which was located in northeast Thailand on the Mekong River.
Officially, it was a Thai military facility. Unofficially, it was a secret US military special operations base.
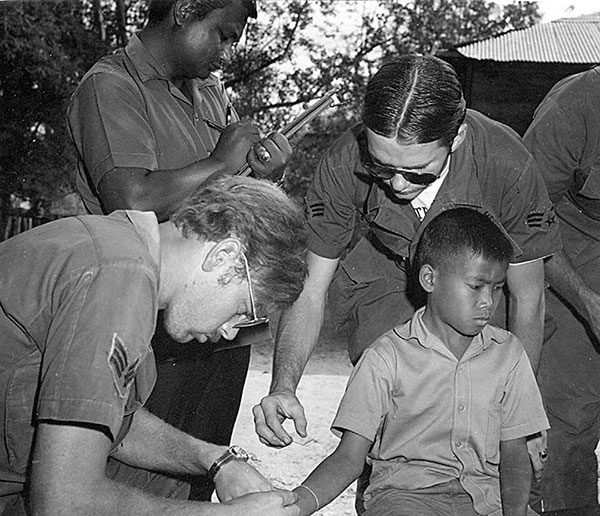
I was an Air Force medic. Like many based there I had a primary duty (working in the hospital ER and flying air-evac), and a secondary one. My secondary was the Medical Civic Action Project (MedCAP) in Nakon Phanom, and neighboring Sakon Nakon Provinces. At least once a week we traveled to remote villages in the provinces to provide villagers with primary medical care they wouldn’t otherwise receive.
Many of the Tha Rae district population are Catholics who emigrated from Vietnam in the early 20th century to escape French colonialism. One of those emigres, after WWI, was a young man born Nguyn Sinh Cung, who changed his name to Ho Chi Minh. Ho lived in Nakon Phanom (NKP) for a couple of years, and his former house there is now a museum.
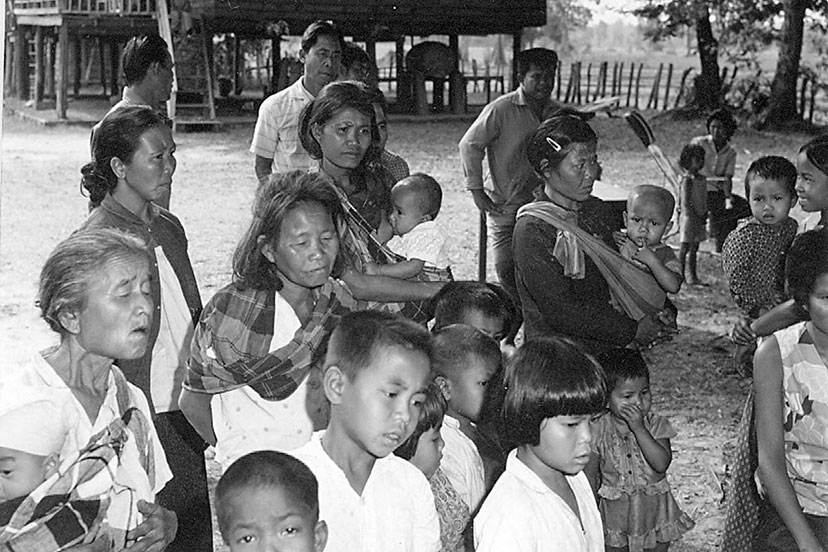
Nakon Phanom, and Sakon Nakon Provinces are 90% rural, and one of the poorest regions in Thailand. It is part of an indigenous sub-region of southeast Asia known a Isaan, which is divided by the Mekong and encompasses most of northeast Thailand and part of western Laos.
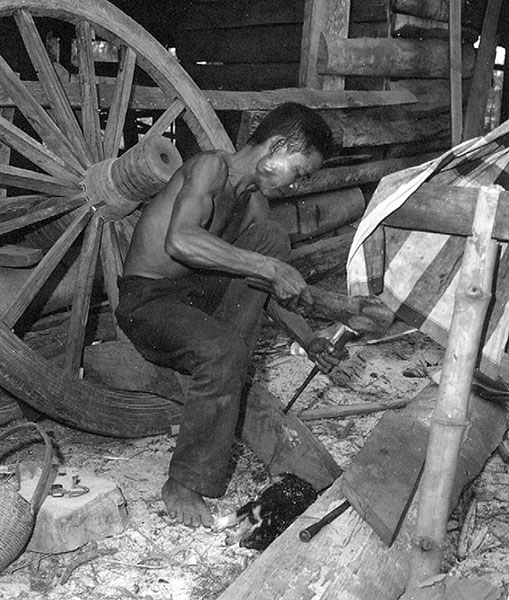
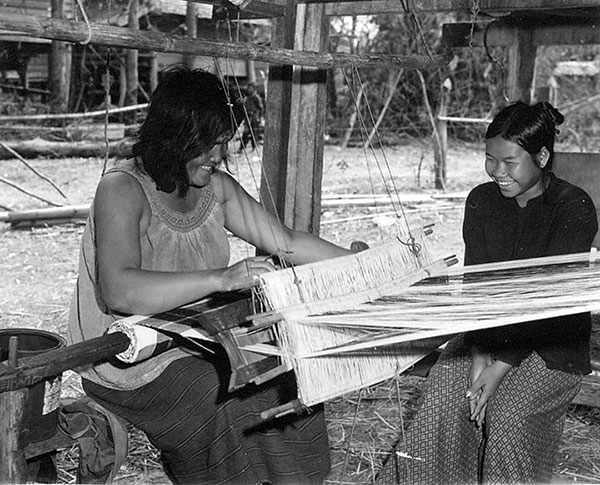
The village economies relied on rice production, cottage industry, and subsistence farming. Very few had running water or electricity. They spoke a distinct dialect that was a mixture of Thai and Lao.

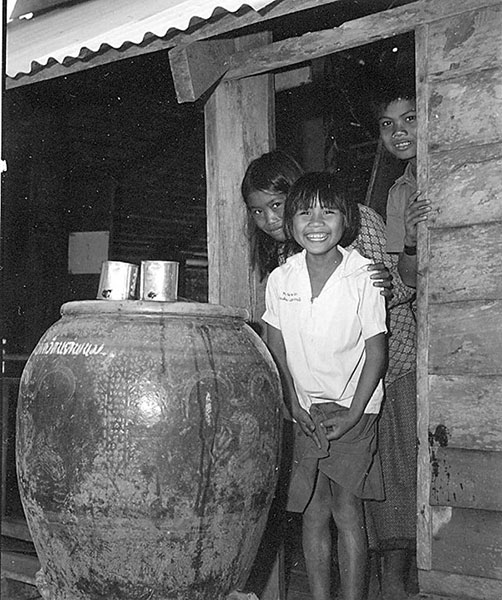
At that time the only hospital, and doctors, in the region were in NKP city – which may as well have been on another continent for most of the rural villagers who had few, if any, motor vehicles. Transportation was primarily by wooden-wheeled carts pulled by water buffalo, as it had been for millennia – or you walked.
Most of the time we drove to the villages. But sometimes for security, due to communist insurgents in the area, we’d go by armed helicopter or Thai navy gunboat on the Mekong River. Fortunately we never encountered any hostile elements – probably because the bad guys knew we were non-combatants on medical missions.
The Thai government medical services in the region’s villages were minimal. I don’t know if that was because they were a cultural minority far removed from the capitol in Bangkok. I do know they were incredibly grateful for the health care provided by the US Air Force. MedCAP was a factor in keeping the communist insurgents from winning the hearts and minds of the rural population.

The villagers expressed their gratitude to us by their hospitality during our visits. It was usually a community event, that often included us having a mid-day feast with the village notables, catered by the moms of the kids. I ate true Thai food long before it became popular in the US.
Usually, as was the local custom, the meal was lubricated with “Lao cao” (akin to American moonshine), which meant we had to get our mission done in the morning. On a couple of occasions we were invited to partake in the local “homegrown”, which would have been rude to refuse. That we made it back to the base after some of those luncheons I attribute to our Thai drivers.
But at least the Lao cao probably killed whatever pathogens we may have picked up from the food. If that didn’t do it, I’m sure the Thai peppers did! (“The Scoville scale measures the common sweet or bell pepper at zero Scoville units since it contains no capsaicin, while the commonly found Thai pepper known locally as prik kee noo logs in at 80,000 to 100,000 Scoville units.”)
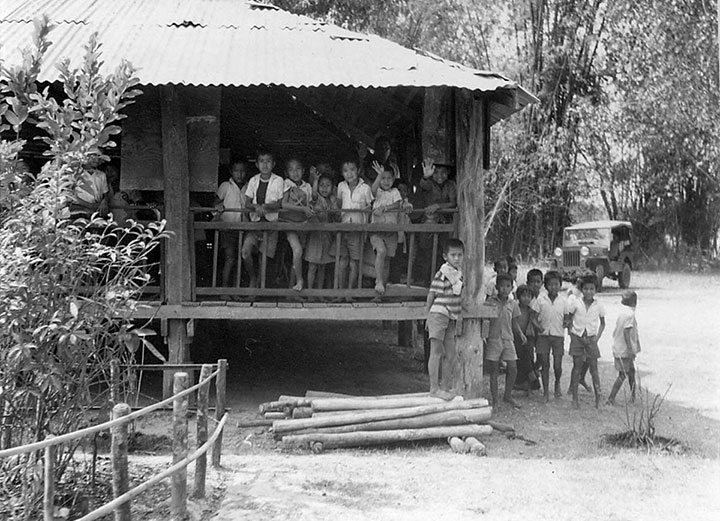
Because the Thai king was dedicated to literacy, one thing the government did provide a lot of to the region was primary schools. Most villages had one, or were within walking distance of one shared by multiple small villages. Because our mission was providing health care to kids, most of our visits were to schools.

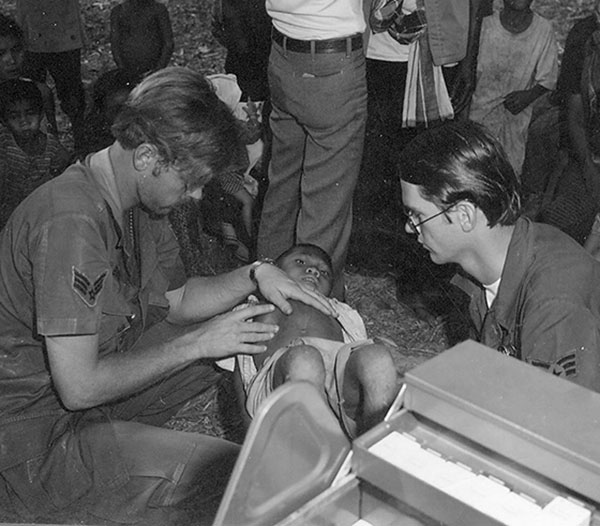
Our focus was twofold. First to provide primary care to the children. Second came pregnant women. Treatment for other adults was usually limited to dental care.
If any adult was actively ill, or had recently suffered an injury, we’d do what we could with the limited resources we brought. On rare occasions we transported a critical case to the hospital in NKP.
Seeing the kids exposed us to childhood maladies largely eradicated in advanced countries. Until you’ve experienced it you don’t realize that even with the deficiencies in our health care system, it was far and away superior to what existed in rural third-world populations at that time.
A common condition in the kids was conjunctiva, which we treated with ointment, then gave the mothers a tube and showed them how to apply it. Other kids had parasites (as did many adults). We’d give them a dose of an anti-parasitic, and a box full to the moms to give once a day.
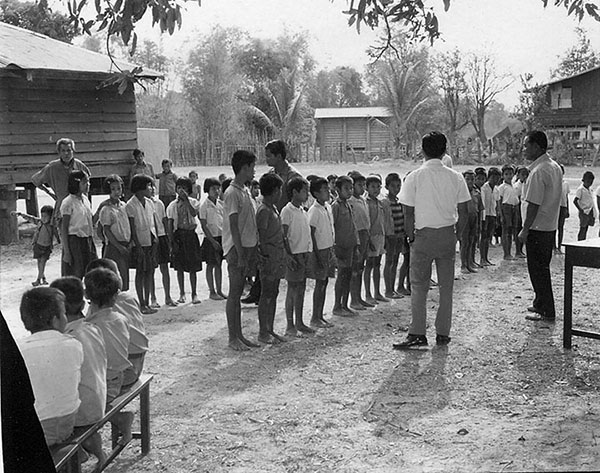
The children lined up for us to see them. They were very well-behaved, but we quickly realized some would try to hustle us. The healthy ones who didn’t get anything from us felt slighted. So when they’d see a child ahead in line get treated, the next couple kids would fabricate the same symptoms.
We handled that scam by giving a box of “special medicine” (multi-vitamins) to those who didn’t actually need any treatment, with instructions to mom to be sure her child took one “every day”. The kid would walk away clutching that box of vitamins – no doubt certain of having put one over on us.
In one village several of the kids had six toes on each foot. I assumed they were birth defects from something in that local environment until one of the Thai air force medics (they translated for us) who was from that region told me it was a genetic trait in some of the indigenous Isaan population. Those with extra toes were considered to be blessed by the spirits.
But some of what we saw was serious. A common problem was water-born infections. Cholera was, and still is, a problem there.
If we encountered an outbreak in a village, that’s one thing that got Thai civilian medical folks seriously involved.
We Americans were vaccinated against cholera. But we also scrupulously avoided drinking the water by bringing our own. When we ate with the villagers, we only consumed what we saw being cooked. (Even with those precautions I got a nasty case of dysentery, that put me out of action for nearly two weeks.)
We’d also see old injuries that didn’t heal properly. Broken limbs were usually treated by the villagers themselves because of severely limited transportation to the hospital. Though some had clear disfigurement from past fractures, we were impressed by how well others had healed.
Rural folk medicine has been in use, successfully, long before what we call modern medicine came about. Most villages had someone, usually a woman, who was the “healer” (for lack of a better term), that learned the arts from a predecessor.
We always made a point of “consulting” with whomever that was in each village. Some of them were impressive in their knowledge of anatomy and physiology without any formal education. They also taught us about using local plants for treatments.
The pregnant women we saw were all given a physical, and at the very least a supply of prenatal vitamins to last them thru delivery. A couple of times our visit to a village coincided with a woman being in labor. Each village had at least one lay midwife with a lot of experience birthing babies, so the only time we’d get involved was if there was complication that put the mother at risk.
I assisted village midwives in two birthings. During my training I’d worked for six months in a hospital labor and delivery unit – but didn’t pretend I was more qualified than an experienced midwife.
Regarding the experience of childbirth, I observed in my training that most American women at their first delivery had only seen birthings in expectant mother class movies – but had never seen a live one. That was a relatively new phenomena to their generation. Many of their mothers, and certainly their grandmothers, had seen birthings before their own first labor, because until post-WWII many babies were still born at home.
By the time the girls in the villages were old enough to have kids, they’d seen many birthings by their mothers, aunts, and other village women. It appeared to me they handled labor more stoically than American women.
Maybe that was because maternal death from childbirth (most often from postpartum infection) was then still too often a fact-of-life in those villages. So if we were present at a birth, we’d give antibiotics to the mother to reduce the infection risk.
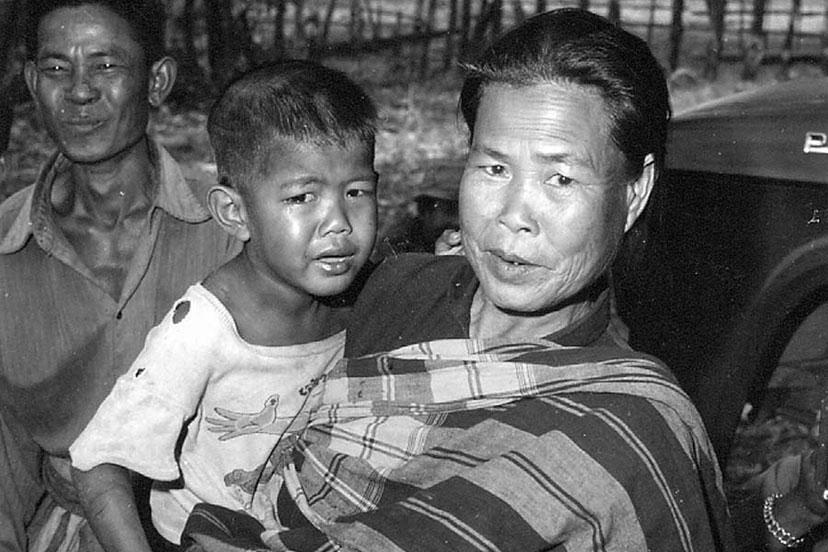
At that time most girls in rural villages were married and started having children in their mid-teens. By their late twenties they’d had multiple pregnancies because the families needed as many kids as possible to help with the work. Repeated pregnancy, combined with working in the rice paddies, aged the women rapidly.
It wasn’t unusual for a woman to birth a child, and the next day be working in the rice paddy with the baby on her back, as village women had been doing since time immemorial. I was impressed. They’d have laughed at the concept of “maternity leave”.
Most of the older women chewed betel nut as a stimulant. But it also darkens the teeth, and causes a variety of dental problems.
I was sympathetic to our dentists having to work in some of those mouths.
Few women from the rural villages avoided that fate, except for some of the most attractive ones. It was common for bar owners from Bangkok, Pattaya, and other cities, to travel into the rural villages to recruit ‘hostesses’. Some girls went voluntarily to escape the villages, but not all.
Female children are a commodity for a subsistence farm family. The girls were not ‘sold’ to the bar owners, because slavery is illegal in Thailand. But the bar owner would ‘loan’ money to the family, and the girl had to work for the owner until the loan was repaid from her earnings – which could take years.
This practice is still going on. Many of the girls working in the Bangkok, Pattaya and Phuket tourist area bars were brought there from rural villages.
We’d encounter the unintended consequences of some of those working relationships in village kids whose parentage was obviously mixed race. Often if a bar girl got pregnant, she’d take the baby back to her village to be raised by her family, then return to the city to continue repaying the family debt. The first time I examined a young Thai child with blue eyes I thought I’d come across another genetic anomaly (like the six toes) until I was told about the likely paternity.
I learned more about the world, and life, in those villages than from all my formal education. That was my “Vietnam war” service. When I wasn’t providing medical care to children in rural villages, I was treating American military personnel in the base hospital ER. I never carried a weapon.
Within six months of my return home from Thailand I was a college student. It was only then that I discovered what a bad person I was for having taken care of those southeast Asian village kids and pregnant women during the war. I heard it from a professor who (upon learning I was Vietnam veteran but not what my job was) asked me how many babies I’d killed.
If you want to know why politics have become so acrimonious today, just look at how the Vietnam anti-war movement treated the veterans. That’s where it started. Civility has gone down hill from there.
Vietnam vets were not thanked for our service in those days. We were spat upon and falsely called baby killers by our self-annointed moral superiors who cared nothing for the truth. The anti-war movement justified it by adopting the radical feminist “All politics is personal!” mantra.
I’m now the President of an international veterans’ organization that is also a charity working in northeast Thailand and Laos. We are not affiliated with any government, have no paid staff (all the work is done by volunteer unpaid veterans) and are funded entirely by private donations.
We’re the same guys who served their during the war – and we still don’t kill babies.