
No two nations are alike when it comes to health care. Over time, each country has settled on a unique mix of policies, service delivery systems, and financing models that work within its resource constraints. Even among high-income nations that have the option to spend more on health care, approaches often vary substantially. These choices affect health system performance in terms of access to care, patients’ experiences with health care, and people’s health outcomes. In this report, we compare the health systems of 11 high-income countries as a means to generate insights about the policies and practices that are associated with superior performance…
With that introduction, authors Eric C. Schneider, Arnav Shah, Michelle M. Doty, Roosa Tikkanen, Katharine Fields, and Reginald D. Williams II, begin their analysis of health care systems in 11 “high-income countries”, in the report Mirror, Mirror 2021 published by the Commonwealth Fund International.
The subtitle: Reflecting Poorly: Health Care in the U.S. Compared to Other High-Income Countries.
The United States does not fare well in this comparison. According to the authors, “The United States trails far behind other high-income countries on measures of health care affordability, administrative efficiency, equity, and outcomes…”
You can download the 39-page report here.

At the Pagosa Springs Town Council’s (rather lengthy) regular meeting on Tuesday evening, August 3, we had a chance to hear from Dr. Rhonda Webb, CEO of the Pagosa Springs Medical Center.
She was addressing, primarily, the financial situation at PSMC, and also introducing the hospital’s strategic plan for 2021-2023. But if you listened ‘between the lines’ Dr. Webb was hinting at a disturbing picture of health care in the United States, coming out of what might be (or might not be?) the worse part of the COVID crisis.
“I’d like to share a few facts about how we get paid at the hospital. A rural hospital system. Medicaid is our state payer; they pay us 60% of what it costs us [to provide a particular service.] Medicare is our federal payer; they pay us 99% of what it costs us [to provide a service.] That will drop to 95% by the end of the year. So 60% of the payers at our hospital pay us less than it costs us to do business. I like to point that out to people so that they’ll know that the health care system, as it is currently built, is broken and needs some adjustment overall, long term.
“PSMC can’t fix it on our own. So the health care costs get pushed to the insurance companies, and the insurance companies, in turn, push those costs onto the people.
“So this is a challenge, and we are trying to navigate through this. And we were already trying to navigate it, before the pandemic ever started…”
Any analysis relies on a set of assumptions. One of the assumptions inherent in Dr. Webb’s analysis, for example, is that PSMC ought to pay its employees — janitors, nurses, clerks, physicians — at rates similar to what they would be paid at other rural hospitals. That is to say, that some employees would be paid $13 per hour, and some would earn $100 per hour (or more). That’s only one of hundreds of assumptions that guide the operations of a typical rural hospital.
Some health care professionals have rejected certain of these assumptions, in an effort to “fix” a broken system. (See this article about Denver physician Dr. P.J. Parmar.)
The authors of the Mirror, Mirror 2021 report likewise began with certain assumptions about how a national health care system ought to operate. Starting with those assumptions, they analyzed 71 ‘performance measures’ across five domains…
- Access to care
- Care process
- Administrative efficiency
- Equity
- Health care outcomes
The data was drawn from Commonwealth Fund international surveys conducted in each country, and administrative data from the Organisation for Economic Co-operation and Development and the World Health Organization.
The 39-page report includes eight graphs that help illustrate the conclusions drawn by the authors. Such as, for example, this one:
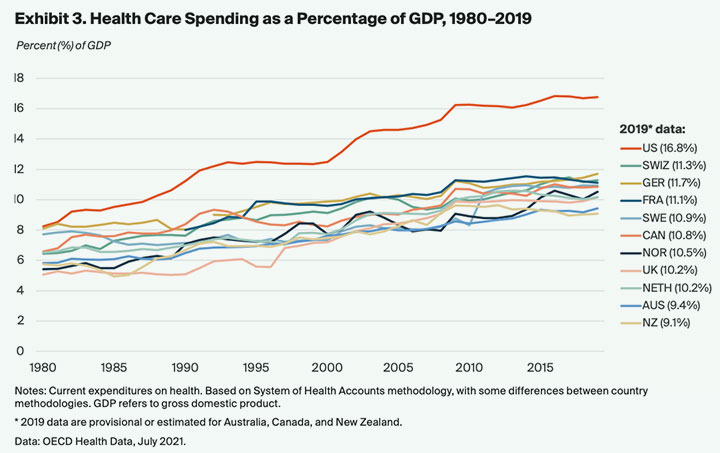
Back in 1980, the cost of health care in United States — relative to the country’s Gross Domestic Product — was pretty much still in the same ballpark as the other ten “high-income” nations included in the Mirror, Mirror report.
As we see, over the next 40 years, the relative cost of health care increased in every one of the countries included in the study. But the relative cost of health care in the United States rose at a dramatically higher rate, to where health care in the US in 2019 — relative to the GDP — is nearly twice as inflated as the other countries in the study.
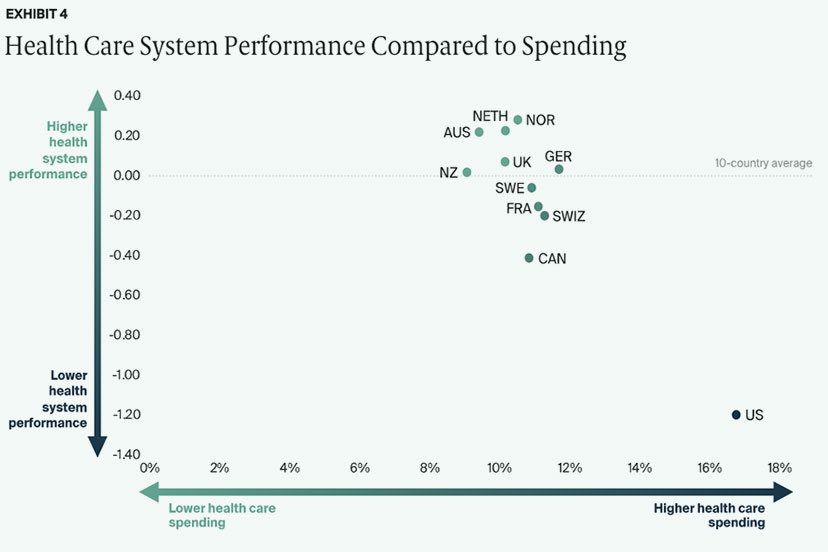
Considering this dramatic increase in health care spending in the US between 1980 and 2019, one might expect that health care outcomes in the United States would be the best in the world. The Mirror, Mirror authors, however, came to basically the opposite conclusion.
The overall health outcomes in the US, taken as a whole, are pitiful in comparison — especially when we consider the cost of health care here.
From the report:
A comparison of the features of top-performing countries and poorer-performing countries suggests that top-performing countries rely on four features to attain better and more equitable health outcomes:
1. They provide for universal coverage and remove cost barriers so people can get care when they need it and in a manner that works for them.
2. They invest in primary care systems to ensure that high-value services are equitably available locally in all communities to all people, reducing the risk of discrimination and unequal treatment.
3. They reduce the administrative burdens on patients and clinicians that cost them time and effort and can discourage access to care, especially for marginalized groups.
4. They invest in social services that increase equitable access to nutrition, education, child care, community safety, housing, transportation, and worker benefits that lead to a healthier population and fewer avoidable demands on health care.
Some type of nationalized health insurance system operates in all of the countries the authors studied, but they concluded that optimum health outcomes require more than ‘insurance coverage’.
Convenient and timely primary care is also vital. Top-ranking countries like the Netherlands and Norway ensure timely availability to care by phone on nights and weekends (with in-person follow-up at home as needed). In the Netherlands, cooperative “GP posts” are staffed by general practitioners (primary care physicians), who are obligated to provide at least 50 hours of after-hours care (between 5:00 pm and 8:00 am) annually in order to maintain their professional licensure. In Norway, the Patients’ Rights Act specifies a right to receive care within specific timeframes and with maximum wait times applying to covered services, including general practitioner visits, hospital care, mental health care, and substance use treatment.
In top-performing countries, workforce policy is geared to ensuring access within communities, especially those that have been historically marginalized. Norway, with the highest number of doctors per person among the 11 countries in our study, has a much larger supply of physicians relative to its population than the U.S. has.
According to Commonwealth Fund data, Norway has about 5 physicians per 1,000 citizens.
The United States has about half that number.
And a broken system?