

This story by Aneri Pattani and Rae Ellen Bichell appeared on Kaiser Health News (KHN) on December 12, 2022. We are sharing it in two installments.
Tim Buck knows by heart how many people died from drug overdoses in his North Carolina county last year: 10. The year before it was 12 — an all-time high.
Those losses reverberate deeply in rural Pamlico County, a tightknit community of 12,000 on the state’s eastern shore. Over the past decade, it has had the highest rate of opioid overdose deaths in North Carolina.
“Most folks know these individuals or know somebody who knows them,” said Buck, the county manager and a lifelong resident, who will proudly tell anyone that four generations of his family have called the area home. “We all feel it and we hate it when our folks hurt.”
Now, the county is receiving money from national settlements with opioid manufacturers and distributors to address the crisis. But by the time those billions of dollars are divided among states and localities, using formulas partially based on population, what trickles down to hard-hit places like Pamlico County can be a trifling sum.
Out of one multibillion-dollar national settlement, Pamlico County is set to receive about $773,000 over nearly two decades. By contrast, Wake County, home to the capital city of Raleigh, is set to receive $36 million during the same period, even though its opioid overdose death rate for the past decade ranked 87th in the state.
Buck said his county’s share “is not a lot of funds per year. But I’m glad we have something to try to reduce that overdose number.”
Rural communities across America were harbingers of the opioid crisis. In the 1990s, misleading marketing by opioid companies helped drive up prescription rates, particularly in coal, lumber, and manufacturing towns across Appalachia and Maine. As painkillers flooded communities, some residents became addicted. Over time, they started using heroin and fentanyl, and the deadly epidemic spilled into suburbs and cities across the nation.
State and local governments filed thousands of lawsuits against drug companies and wholesalers accused of fueling the crisis, resulting in a plethora of settlement deals. The largest to date is a $26 billion settlement that began paying out this year.
As the funds arrive, some people say it’s reasonable for densely populated cities and counties to receive more, as they serve a greater number of residents. But others worry such an approach misses an opportunity to use that money to make a difference in rural communities that have been disproportionately affected for decades.
“You could really diminish what is effectively generational, more than 20 years of harm in rural areas,” said Robert Pack, co-director of East Tennessee State University’s Addiction Science Center.
Just because rural areas are less populated doesn’t mean it’s cheaper to provide health services there. Research suggests the per-person cost can be greater when counties can’t capitalize on economies of scale.
In West Virginia, Attorney General Patrick Morrisey has rejected several national opioid settlements because of their distribution methods and pursued separate lawsuits instead, saying the state needs a deal that reflects the severity of its crisis, not the size of its population.
Allocations from the $26 billion national settlement were determined by each state’s population and the portion of overdose deaths, residents with opioid use disorders, and prescription painkillers it contributed to the nation’s total. Many states used similar formulas to distribute funds among their cities and counties.
Although the goal was to reflect the severity of each area’s crisis, those statistics tend to scale up by population. Further, some experts say wealthier communities with higher rates of prescription drug use may benefit while poorer communities affected by heroin and fentanyl may lose out.
Pennsylvania took a different route, devising its own formula to distribute funds among 67 counties — taking into account opioid-related hospitalizations and first responders’ administration of naloxone, an overdose reversal medication. When that formula left 11 rural counties without “enough money to make an impact,” the state decided each county would receive a minimum of $1 million over the 18-year settlement period, said Glenn Sterner, an assistant professor at Penn State who helped develop the state formula and co-authored a paper on it.
In other parts of the country without guaranteed minimums, some local officials say their share of the settlement funds won’t cover one psychologist’s salary, let alone the creation of treatment facilities.
But medical treatment — among the most expensive interventions — is just one piece of the puzzle, said Nidhi Sachdeva, who leads health and opioid initiatives for the North Carolina Association of County Commissioners. She recommends that rural counties explore lower-cost, evidence-based options like distributing naloxone, funding syringe service programs, or connecting people to housing or employment.
Another option is to pool resources among counties. In eastern North Carolina, Martin, Tyrrell, and Washington counties plan to funnel their settlement dollars into a long-standing regional health department, said David Clegg, manager and attorney for Tyrrell County. With a combined population of 36,000, the three counties have used a similar approach in combating COVID-19 and sexually transmitted infections.
When it comes to funding, “we’re always the caboose of the train,” Clegg said of his county. “We couldn’t function if we didn’t partner for lots of different services.”
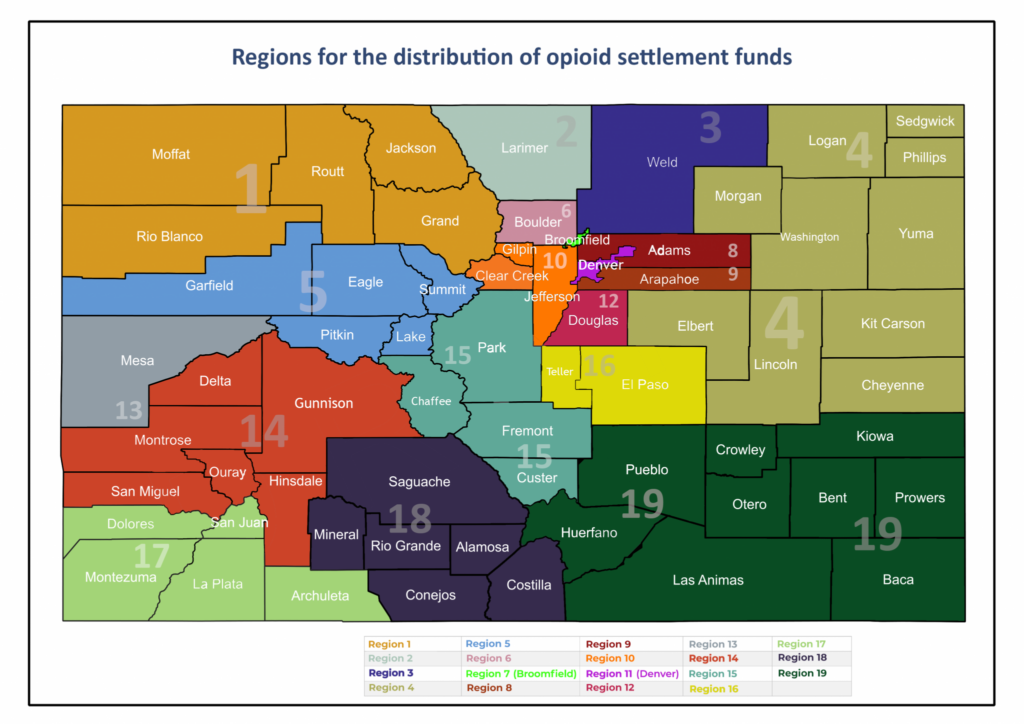
In Colorado, pooling funds is built into the state’s model for managing opioid settlement money. The lion’s share of funds is going to 19 newly formed regions, about half of which comprise multiple counties…
{kind=link}