
The Colorado Department of Education (CDE) released its latest “guidance” earlier this week, laying out suggestions and requirements for schools and school districts as they prepare to start the 2020-2021 school year within a few weeks. You can download the 18-page guidance PDF here.
The CDE’s five key goals… with my comments…
1. Maximize in-person learning in as safe and healthy way as possible.
We have made a shared cultural decision that all children must learn certain intellectual and practical skills, and that we prefer they learn these skills in a school classroom of 20-30 same-aged children, with a paid adult teacher leading the process. This is, of course, not how children learned necessary skills and lessons through most of human history, in most cultures, but we now generally believe it’s the best way, and we’ve built our families and social structures around this arrangement.
How to adjust this structure to keep people reasonably safe and healthy during the global spread of a contagious disease? That’s basically what the CDE guidance attempts to address.
2. Ensure a reasonable level of safety for students and staff for in-person learning.
This seems to be a repeat of Number 1, phrased slightly differently. Goal Number 1 says, “as safe and healthy as possible.”
Goal Number 2 uses the term “reasonable.” So, what is “reasonable”?
The expectation of zero transmission among students and staff is not reasonable. If we operate schools in anything approaching the traditional manner, there will be transmission of disease this school year. How much transmission is “reasonable”? We’ll consider that in a moment.
3. Minimize disruptions to education by facilitating timely responses to COVID-19 through cohorting students and staff when possible, screening for symptomatic individuals, and coordinating closely with local and state public health agencies.
“Cohorting students” as suggested by CDE (and many others) means that a class of, say, 25 students, will operate as a unit and have very little contact with any other student unit. Student in each unit will keep mostly to certain fixed indoor spaces; will eat lunch in the classroom; will exercise and conduct recess separately from other units; and will interact with only certain staff members.
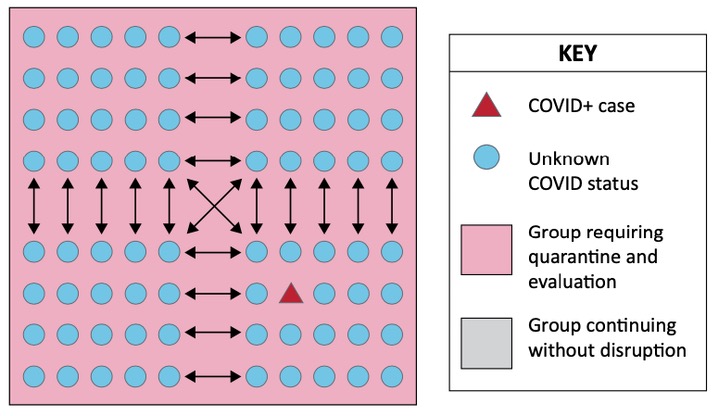
When an infected individual is allowed to be in contact with people outside his/her cohort — during recess, in the lunch room, in the auditorium, on sports teams — it becomes much more difficult to evaluate and control the spread.
The CDE document illustrates the value of “cohorts” with these two graphs, showing a single individual who tests positive for COVID:
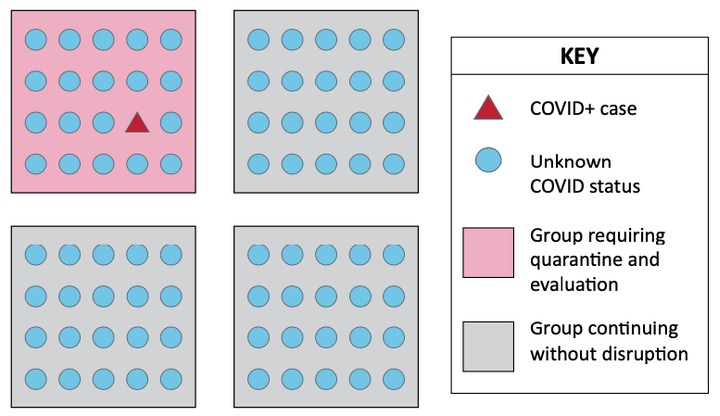
We might note, in the above illustration, that everyone other than the COVID-positive case is assumed to have “Unknown COVID Status”. A label with some significance, as we will see, because the COVID status of almost everyone in a school building will typically remain “Unknown”. Or so it would appear.
The other piece of this Goal that I find interesting is “screening for symptomatic individuals.” More about that in a moment.
4. Ensure equity in educational opportunity by considering learning and health needs of all students, including those with varying health conditions, economic backgrounds, language skills, or educational needs.
This goal needs no comment.
5. Encourage flexibility, adaptation, and innovation as schools develop novel approaches to disease control appropriate to local contexts and as scientific knowledge about COVID-19 transmission and control develops.
It’s clear that ‘scientific knowledge’ about COVID-19 transmission and control as been ‘developing’ for a while now, and will continue to ‘develop.’ The guidance from CDE does not, however, appear to encourage a high degree of flexibility or innovation. Instead, it appears to specify 18 pages of specific protective actions, such as (for example):
- Regularly clean and disinfect all high-touch surfaces and shared objects…
- Require face coverings over the nose and mouth for all staff, including during in-person instruction… If necessary, the mask may be removed for instruction for the shortest duration possible…
- Require cloth face coverings over the nose and mouth for students ages 11 and older except during outdoor recess and exercise activities where appropriate distancing can be maintained, unless the student has a health or education reason for not wearing a mask…
- Students will undergo home temperature and symptom screening or self-screening…
- Remain home if experiencing symptoms of COVID-19 or if a family member or other close contact has been diagnosed with COVID-19 or is experiencing symptoms…
- Teachers and other adult staff should make the greatest effort to adhere to 6-foot distancing, as their risk and disease transmission potential is higher than students…
Not one of the dozens of actions recommended by the CDE — practiced by itself — can do much to slow the spread of a contagious disease in a school full of children and adults.
But the public health official I spoke to at San Juan Basin Public Health this week — Brian Devine, planning and logistics section chief — suggested that, practiced all together, these protective measures are capable of providing a “reasonably safe” environment in a public school.

Mr. Devine and I also discussed a rather sticky subject: “screening for symptomatic individuals.” The CDE guidance is built largely around the idea that COVID-positive cases can be identified through an evaluation of symptoms. A child who shows up at school with a fever, or a dry cough, or who develops such symptoms during the day, will — under the published guidance — be immediately isolated, and sent home, and people who had close contact with this child will be advised to isolate themselves.
One little problem. Infected individuals do not always develop symptoms. In fact, according to a June 16 article in the scientific journal, Nature, only about 20 percent of children who become infected with the SARS-CoV-2 virus develop recognizable symptoms. Four out of five infected children experience COVID as nothing more serious than an ordinary runny nose — that is, as unremarkable, even unnoticeable.
But these four-out-of-five asymptomatic children are still able to transmit the infection to others.